Oronasal and Orosinusal Lesions Associated with Intranasal Cocaine Use: Two Clinical Case Reports
Article Sidebar
Main Article Content
Abstract
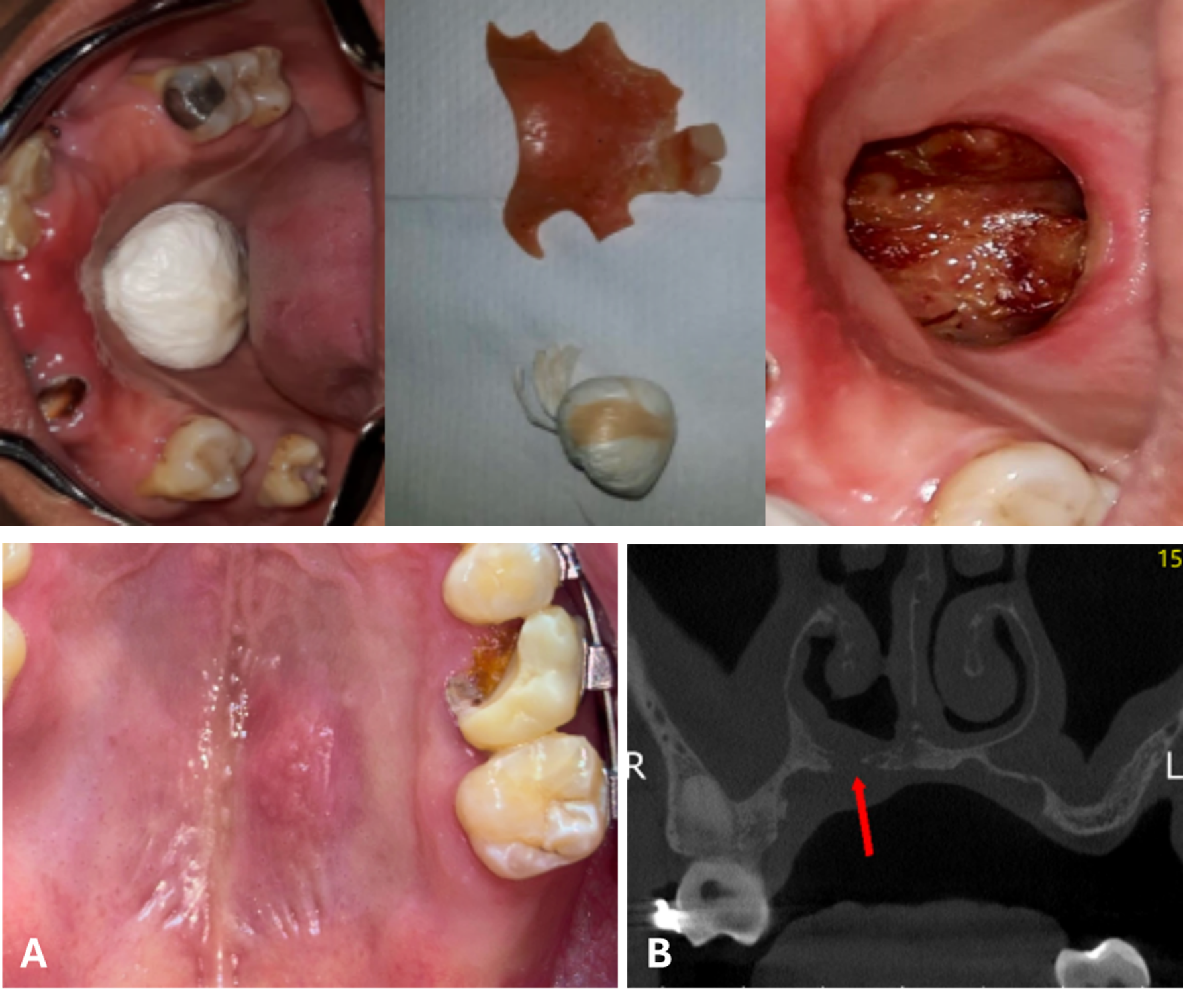
Intranasal cocaine use may lead to a progressive spectrum of centrofacial destruction known as cocaine-induced midline destructive lesion (CIMDL), which may involve the hard palate and result in oronasal or orosinusal communication, with major functional and social repercussions. Because oral examination routinely exposes the palate, dentists may be the first clinicians to detect these lesions; however, diagnosis is often delayed because patients may initially omit illicit drug use and because the clinical presentation may overlap with vasculitic, infectious, and neoplastic disorders. This report describes two cases of cocaine-associated palatal destruction diagnosed at different stages of progression and discusses the main etiopathogenic, histopathological, diagnostic, and therapeutic aspects relevant to dental practice. The first case involved a woman with an established palatal perforation measuring approximately 3 cm, hypernasal speech, nasal regurgitation of food and liquids, and improvised self-occlusion of the defect with plastic material. The second case involved a 35-year-old man with a posterior palatal nodule, computed tomographic evidence of osteolysis affecting the floor of the nasal cavity, and incisional biopsy showing chronic granulomatous inflammation in the context of chronic intranasal cocaine use. Together, these cases illustrate that cocaine-related palatal destruction may be identified at markedly different points along the same pathological continuum, from pre-perforative osteolytic disease to extensive communication with severe functional impairment. Early recognition, structured differential diagnosis, cocaine cessation, and multidisciplinary rehabilitation are essential for appropriate management.
Article Details

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain the copyright of their articles and grant the journal the right of first publication under the Creative Commons Attribution (CC BY) license, which allows others to share and adapt the work with proper attribution.
References
United Nations Office on Drugs and Crime. World Drug Report 2022. Vienna: UNODC; 2022.
United Nations Office on Drugs and Crime. World Drug Report 2020. Vienna: UNODC; 2020.
Abdalla RR, Madruga CS, Ribeiro M, Pinsky I, Caetano R, Laranjeira R. Prevalence of cocaine use in Brazil: data from the II Brazilian national alcohol and drugs survey (BNADS). Addict Behav. 2014;39(2):297-301.
Trimarchi M, Bussi M, Sinico RA, Meroni P, Specks U. Cocaine-induced midline destructive lesions: an autoimmune disease? Autoimmun Rev. 2013;12(4):496-500.
Silvestre FJ, Salort-Llorca C, Mínguez-Serra MP, Silvestre-Rangil J. Cocaine-related oronasal communication and hard palate destruction. J Investig Clin Dent. 2012;3(3):157-160.
Wiesner O, Russell KA, Lee AS, Jenne DE, Trimarchi M, Gregorini G, Smith KG, et al. Antineutrophil cytoplasmic antibodies reacting with human neutrophil elastase as a diagnostic marker for cocaine-induced midline destructive lesions but not au-toimmune vasculitis. Arthritis Rheum. 2004;50(9):2954-2965.
Brand HS, Gonggrijp S, Blanksma CJ. Cocaine and oral health. Br Dent J. 2008;204(7):365-369.
Trimarchi M, Gregorini G, Facchetti F, Morassi ML, Manfredini C, Maroldi R, Nicolai P, Russell KA, McDonald TJ, Specks U. Cocaine-induced midline destructive lesions: clinical, radiographic, histopathologic, and serologic features and their diffe-rentiation from Wegener granulomatosis. Medicine (Baltimore). 2001;80(6):391-404.
Nitro L, Accorona R, Nava MB, Brusati R, Chiapasco M, Moneghini L, Biglioli F, Stucchi G, Trimarchi M. Distribution of cocaine-induced midline destructive lesions: systematic review and classification. Eur Arch Otorhinolaryngol. 2022;279(5):2543-2552. doi: https://doi.org/10.1007/s00405-022-07255-6.
Capparé P, Vinci R, Gherlone EF, Ferrini F. Cocaine-induced midline destructive lesions: a real challenge in oral rehabilita-tion. Int J Environ Res Public Health. 2021;18(6):3219. doi: https://doi.org/10.3390/ijerph18063219.
Silvestre FJ, Pérez-Herbera A, Puente-Sandoval A, Bagán JV. Hard palate perforation in cocaine abusers: a systematic review. Clin Oral Investig. 2010;14(6):621-628. doi: https://doi.org/10.1007/s00784-009-0346-9.
Trimarchi M, Miluzio A, Nicolai P, Porta A, Bussi M, Marchetti A. Massive apoptosis erodes the quiescent mucosa of cocai-ne-addicted patients. Am J Rhinol. 2006;20(2):200-204.
Midyat L, Enver N, Günhan Ö, Tuncel A. Differentiation of cocaine-induced midline destructive lesions from ANCA-associated vasculitis. Case Rep Med. 2018;2018:7603286. doi: https://doi.org/10.1155/2018/7603286.
Trimarchi M, Bussi M. Cocaine-induced midline destructive lesions (CIMDL): an update on pathogenesis and treatment. Rhinology. 2020;58(5):411-420. doi: https://doi.org/10.4193/Rhin20.048.
Espinoza LR, Perez AR. Cocaine-induced vasculitis: clinical and immunological spectrum. Curr Rheumatol Rep. 2012;14(6):532-538. doi: https://doi.org/10.1007/s11926-012-0285-0.
Pearson T, Bremmer M, Cohen J, Driscoll M. Vasculopathy related to cocaine adulterated with levamisole: a review of the literature. Dermatol Online J. 2012;18(7):1.
McGrath MM, Isakova T, Rennke HG, Mottola AM, Laliberte KA, Niles JL. Contaminated cocaine and antineutrophil cyto-plasmic antibody-associated disease. Clin J Am Soc Nephrol. 2011;6(12):2799-2805. doi: https://doi.org/10.2215/CJN.01540211.
Strambu V, Paduraru DN, Ion D. Cocaine-induced vasculitis associated with levamisole adulteration: current evidence. Curr Treat Options Rheumatol. 2024;10:45-61. doi: https://doi.org/10.1007/s40674-024-00219-7.
Trimarchi M, Sinico RA, Teggi R, Bussi M, Specks U, Meroni PL. Otorhinolaryngological manifestations in granulomatosis with polyangiitis. Autoimmun Rev. 2013;12(4):501-505. doi: https://doi.org/10.1016/j.autrev.2012.08.010.
Crovetto-Martínez R, Aguirre-Urizar JM, Orte-Aldea C, Araluce-Iturbe I, Whyte-Orozco J, Crovetto-De la Torre MA. Muco-cutaneous leishmaniasis must be included in the differential diagnosis of midline destructive disease: two case reports. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;119(1):e20-e26. doi: https://doi.org/10.1016/j.oooo.2014.10.005.
Trimarchi M, Bussi M, Sinico RA, Meroni P. Palate perforation differentiates cocaine-induced midline destructive lesions from granulomatosis with polyangiitis. Acta Otorhinolaryngol Ital. 2017;37(4):281-285. doi: https://doi.org/10.14639/0392-100X-1374.
Green RJ, Gardiner Q, Vinod K. A case series and literature review on patients with rhinological complications secondary to the use of cocaine and levamisole. J Laryngol Otol. 2020;134(5):440-446. doi: https://doi.org/10.1017/S0022215120000705.
Melo CAA, Guimarães HRG, Medeiros RCF, Souza GCA, Santos PBD, Tôrres ACSP. Oral changes in cocaine abusers: an integrative review. Braz J Otorhinolaryngol. 2022;88(4):633-641. doi: https://doi.org/10.1016/j.bjorl.2021.01.009.
Colletti G, Allevi F, Valassina D, Bertossi D, Biglioli F. Repair of cocaine-related oronasal fistula with forearm radial free flap. J Craniofac Surg. 2013;24(5):1734-1738. doi: https://doi.org/10.1097/SCS.0b013e31829405e0.
Berberi AN, Moukarzel MA, Finianos M. Oral rehabilitation for a patient with cocaine-induced midline destructive lesions. Case Rep Otolaryngol. 2024;2024:7109261. doi: https://doi.org/10.1155/2024/7109261.
Di Cosola M, Turco M, Acero J, Navarro-Vila C, Cortelazzi R. Cocaine-related syndrome and palatal reconstruction: report of a series of cases. Int J Oral Maxillofac Surg. 2007;36(8):721-727. doi: https://doi.org/10.1016/j.ijom.2007.03.015.
Palmero-Sánchez B, Faelens G, Corriols-Noval P, López-Simón E, Morales-Angulo C. Cocaine-induced oronasal communi-cation of the midline of the palate: a case report. Medwave. 2024;24(2):e2883. doi: https://doi.org/10.5867/medwave.2024.02.2883.