Carcinoma Adrenocortical Metastático Simulando Feocromocitoma: O Custo Potencialmente Fatal de Negligenciar o Julgamento Clínico
Barra lateral de artigos
Conteúdo do artigo principal
Resumo
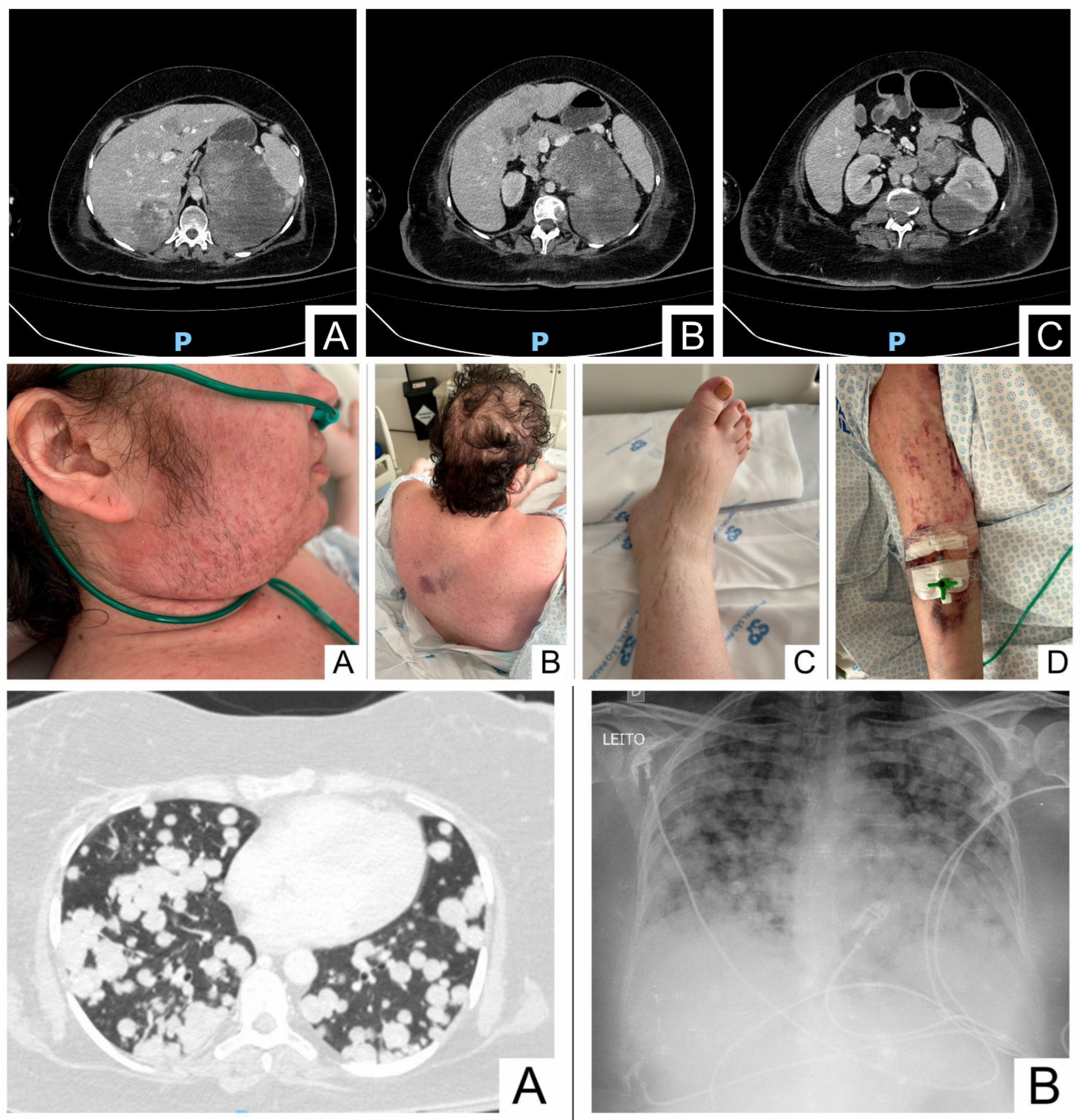
O carcinoma adrenocortical (ACC) é uma neoplasia endócrina rara e agressiva, com prognóstico desfavorável. Suas apresentações clínicas heterogêneas frequentemente mimetizam distúrbios endócrinos mais comuns, como síndrome dos ovários policísticos, síndrome de Cushing (SC), disfunção tireoidiana ou feocromocitoma, levando a erros diagnósticos e atraso no tratamento. Este relato descreve uma mulher de 34 anos que, apesar de apresentar fenótipo de SC, virilização, uma massa adrenal esquerda de 11 × 9 × 8 cm e múltiplas lesões pulmonares e hepáticas, foi inicialmente diagnosticada com feocromocitoma metastático com base exclusivamente em achados de imagem e biópsia hepática. Somente após encaminhamento a um centro terciário, a paciente, com apresentação clínica e perfil bioquímico indistinguíveis, foi identificada como portadora de ACC, diagnóstico posteriormente confirmado por meio de revisão detalhada da biópsia hepática. Infelizmente, devido ao estágio avançado da doença, foi conduzida com cuidados paliativos até seu óbito, duas semanas após a admissão. Este relato ressalta a importância fundamental do julgamento clínico no diagnóstico, enfatizando que exames de imagem e o cuidado fragmentado nunca devem substituir uma avaliação clínica abrangente. Mesmo com ferramentas diagnósticas avançadas, a avaliação clínica completa permanece essencial. A interpretação inadequada de exames de imagem, laboratoriais e histopatológicos, sem considerar o contexto clínico, pode resultar em atrasos diagnósticos e desfechos desfavoráveis, especialmente em doenças endócrinas raras e graves como o ACC.
Detalhes do artigo

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Authors retain the copyright of their articles and grant the journal the right of first publication under the Creative Commons Attribution (CC BY) license, which allows others to share and adapt the work with proper attribution.
Referências
Fassnacht M, Assie G, Baudin E, Eisenhofer G, de la Fouchardiere C, Haak HR, de Krijger R, Porpiglia F, Terzolo M, Berruti A. Adrenocortical carcinomas and malignant phaeochromocytomas: ESMO-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020 Nov;31:1476–90. doi:10.1016/j.annonc.2020.08.2099.
Fassnacht M, Puglisi S, Kimpel O, Terzolo M. Adrenocortical carcinoma: a practical guide for clinicians. Lancet Diabetes Endo-crinol. 2025 May;13:438–52. doi:10.1016/S2213-8587(24)00378-4.
Ziqin L, Yurui W, Xiaobo C, Jing L, Yuzhu L. Delayed identification of adolescent adrenal cortical carcinoma initially diagnosed as polycystic ovary syndrome. J Pediatr Adolesc Gynecol. 2021 Oct;34:764–7. doi:10.1016/j.jpag.2021.03.004.
Alharbi TAF, Rababa M, Alsuwayl H, Alsubail A, Alenizi WS. Diagnostic challenges and patient safety: the critical role of accuracy - a systematic review. J Multidiscip Healthc. 2025 May;18:3051–64. doi:10.2147/JMDH.S512254.
Ferriman D, Gallwey JD. Clinical assessment of body hair growth in women. J Clin Endocrinol Metab. 1961 Nov;21:1440–7. doi:10.1210/jcem-21-11-1440.
Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, Carbone PP. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982 Dec;5:649–55.
Friendlander AH, Ettinger RL. Karnofsky performance status scale. Spec Care Dentist. 2009 Jul-Aug;29:147–8. doi:10.1111/j.1754-4505.2009.00088.x.
Antonini SR, Leal LF, Cavalcanti MM. Pediatric adrenocortical tumors: diagnosis, management and advancements in the un-derstanding of the genetic basis and therapeutic implications. Expert Rev Endocrinol Metab. 2014 Sep;9(5):445–64. doi:10.1586/17446651.2014.941813.
Hatano M, Takenaka Y, Inoue I, Homma K, Hasegawa T, Sasano H, Awata T, Katayama S. Feminizing adrenocortical carcinoma with distinct histopathological findings. Intern Med. 2016;55:3301–7. doi:10.2169/internalmedicine.55.5912.
Dhir G, Jain V, Merritt A. Thyroid disorders. Prim Care. 2024 Sep;51:405–15. doi:10.1016/j.pop.2024.04.001.
Schwarz C, Leichtle AB, Arampatzis S, Fiedler GM, Zimmermann H, Exadaktylos AK, Lindner G. Thyroid function and serum electrolytes: does an association really exist? Swiss Med Wkly. 2012 Sep;142:w13669. doi:10.4414/smw.2012.13669.
Saraiva M, da Inez Correia R, Azevedo SX, Brandão JR, Oliveira JC, Palma I. ACTH-producing adrenocortical carcinoma: an exceedingly rare diagnosis. J Egypt Natl Cancer Inst. 2024 Jul;36:24. doi:10.1186/s43046-024-00229-z.
Dilrukshi MDSA, Wickramarachchi AW, Abeyaratne DDK, Shine B, Jafar-Mohammadi B, Somasundaram NP. An adrenocortical carcinoma associated with non-islet cell tumor hypoglycemia and aberrant ACTH production. Case Rep Endocrinol. 2020 Mar;2020:2025631. doi:10.1155/2020/2025631.
Araujo-Castro M, Marazuela M. Cushing’s syndrome due to bilateral adrenal cortical disease: bilateral macronodular adrenal cortical disease and bilateral micronodular adrenal cortical disease. Front Endocrinol. 2022 Aug;13:913253. doi:10.3389/fendo.2022.913253.
Charchar HLS, Fragoso MCBV. An overview of the heterogeneous causes of Cushing syndrome resulting from primary macronodular adrenal hyperplasia (PMAH). J Endocr Soc. 2022 Mar;6:bvac041. doi:10.1210/jendso/bvac041.
Mete O, Juhlin CC. Recent progress in the pathologic classification of pheochromocytomas and paragangliomas. Best Pract Res Clin Endocrinol Metab. 2024 Dec;38:101958. doi:10.1016/j.beem.2024.101958.
Yener S, Demir L, Demirpence M, Mahmut Baris M, Simsir IY, Ozisik S, Comlekci A, Demir T. Interference in ACTH immu-noassay negatively impacts the management of subclinical hypercortisolism. Endocrine. 2017 May;56:308–16. doi:10.1007/s12020-017-1268-7.
Donegan DM, Algeciras-Schimnich A, Hamidi O, Young WF, Nippoldt T, Bancos I, Erickson D. Corticotropin hormone assay interference: a case series. Clin Biochem. 2019 Jan;63:143–7. doi:10.1016/j.clinbiochem.2018.11.006.
Fassnacht M, Tsagarakis S, Terzolo M, Tabarin A, Sahdev A, Newell-Price J, Pelsma I, Marina L, Lorenz K, Bancos I, Arlt W, Dekkers OM. European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2023 Jul;189(1):G1–G42. doi:10.1093/ejendo/lvad066.
La Rosa S. Diagnostic, prognostic, and predictive role of Ki67 proliferative index in neuroendocrine and endocrine neoplasms: past, present, and future. Endocr Pathol. 2023 Mar;34(1):79–97. doi:10.1007/s12022-023-09755-3.
Zhang H, Bu H, Chen H, Wei B, Liu W, Guo J, Li F, Liao D, Tang Y, Zhang Z. Comparison of immunohistochemical markers in the differential diagnosis of adrenocortical tumors: immunohistochemical analysis of adrenocortical tumors. Appl Im-munohistochem Mol Morphol. 2008 Jan;16:32–9. doi:10.1097/PAI.0b013e318032cf56.
Perrino CM, Ho A, Dall CP, Zynger DL. Utility of GATA3 in the differential diagnosis of pheochromocytoma. Histopathology. 2017 Sep;71:475–9. doi:10.1111/his.13229.
Grubbs E, Lee JE. Limited prognostic value of the 2004 International Union Against Cancer staging classification for adreno-cortical carcinoma: proposal for a revised TNM classification. Cancer. 2009 Oct;115:5847–5847. doi:10.1002/cncr.24693.