Hodgkin Lymphoma - A Rare Neoplasm with Diagnostic and Therapeutic Challenges
Article Sidebar
Main Article Content
Abstract
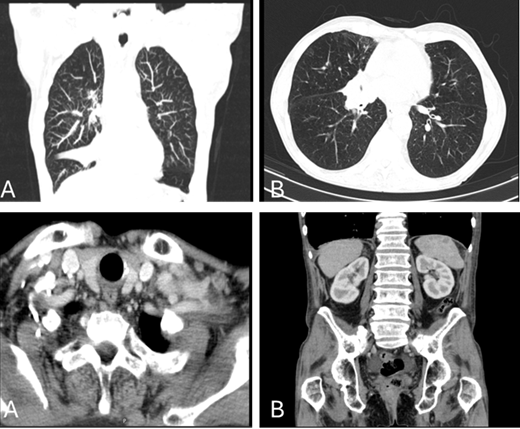
The Classical Hodgkin Lymphoma (CHL) had four subgroups: nodular sclerosis, mixed cellularity, lymphocyte-rich and lymphocyte-depleted. Clinical diagnosis can be difficult because the symptoms are like other diseases. Lymphadenopathies and B symptoms may allow a diagnosis of suspicion, which must be confirmed by lymph node biopsy. One of its key features is the presence of mononucleated and multinucleated cells, the Hodgkin and Reed Sternberg cells. Chemotherapy (QT) ABVD (adriamycin, bleomycin, vinblastine, dacarbazine) is considered the standard therapy. The follow-up is very important due to the relapse risk and the potential late toxicity. The authors report a rare case of cHL nodular sclerosis IV-A, International Prognostic Score (IPS) 5 diagnosed by excisional biopsy of adenomegaly of the left armpit. The 18F-fluorodeoxyglucose positron emission tomography (18F-FDG PET) revealed a good response after QT. A rare bleomycin pulmonary toxicity was diagnosed, and he died. This paper aims to review the current knowledge concerning CHL.
Article Details

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain the copyright of their articles and grant the journal the right of first publication under the Creative Commons Attribution (CC BY) license, which allows others to share and adapt the work with proper attribution.
References
Falini B, Martino G, Lazzi S. A comparison of the International Consensus and 5th World Health Organization classifications of mature B-cell lymphomas. Leukemia. 2023;37:18–34. https://doi.org/10.1038/s41375-022-01764-1.
Alaggio R, Amador C, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022;36:1720–1748. https://doi.org/10.1038/s41375-022-01620-2.
Hoppe R, Advani R, et al. NCCN Clinical Practice Guidelines in Oncology: Hodgkin Lymphoma. Version 2.2025 — June 10, 2025.
Eichenauer DA, Aleman BMP, Andre M, Federico M, Hutchings M, Illidge T, Engert A, Ladetto M. Hodgkin lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv19–iv29. doi:10.1093/annonc/mdy080.
Pinto AAC, et al. Linfoma Hodgkin clássico subtipo esclerose nodular. Hematol Transfus Cell Ther. 2024;46(S4):S1–S1267.
Jarrett RF. Viruses and Hodgkin’s lymphoma. Ann Oncol. 2002;13(Suppl 1):23–29.
Mani H, Jaffe ES. Hodgkin lymphoma: an update on its biology with new insights into classification. Clin Lymphoma Myeloma. 2009;9:206–216.
Hjalgrim H, Smedby KE, Rostgaard K, et al. Infectious mononucleosis, childhood social environment, and risk of Hodgkin lymphoma. Cancer Res. 2007;67:2382–2388.
Jarrett RF, et al. Impact of tumor Epstein–Barr virus status on presenting features and outcome in age-defined subgroups of patients with classic Hodgkin lymphoma: a population-based study. Blood. 2005;106:2444–2451.
Carbone A, Gloghini A. Aids-related lymphomas: from pathogenesis to pathology. Br J Haematol. 2005;130:662–670.
Landgren O, Gilbert ES, Rizzo JD, et al. Risk factors for lymphoproliferative disorders after allogeneic hematopoietic cell transplantation. Blood. 2009;113:4992–5001.
Landgren O, et al. Autoimmunity and susceptibility to Hodgkin lymphoma: a population-based case-control study in Scan-dinavia. J Natl Cancer Inst. 2006;98:1321–1330.
Schnitzer B. Hodgkin Lymphoma. Hematol Oncol Clin North Am. 2009;23:747–768.
Melo LJ, Goulart G, et al. Linfoma Hodgkin clássico variante esclerose nodular localização mediastinal. Hematol Transfus Cell Ther. 2024;46(S4):S1–S1267.
Forteza-Vila J, Fraga M. Differential diagnosis of classic Hodgkin lymphoma. Int J Surg Pathol. 2010;18(3 Suppl):124S–127S.
Gobbi PG, et al. Hodgkin lymphoma. Crit Rev Oncol Hematol. 2012. http://dx.doi.org/10.1016/j.critrevonc.2012.07.002.
Connors JM. Clinical manifestations and natural history of Hodgkin’s lymphoma. Cancer J. 2009;15:124–128.
Hoppe RT, Advani RH, et al. Hodgkin lymphoma, version 2.2012 featured updates to the NCCN guidelines. J Natl Compr Canc Netw. 2012;10(5):589–597.
Stein H, et al. Hodgkin lymphoma. In: Swerdlow SH, Campo E, Harris NL, et al., editors. WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon, France: IARC Press; 2008. p. 321–334.
Townsend W, Linch D. Hodgkin's lymphoma in adults. Lancet. 2012;380:836–847.
Blum KA. Upcoming diagnostic and therapeutic development in classical Hodgkin's lymphoma. Hematology Am Soc He-matol Educ Program. 2010:93–100.
Is there any place for the allogeneic transplant in classic Hodgkin’s lymphoma in the checkpoint inhibitors era? Hematologia. 2018;22(Suppl):23–29.
Hodgkin’s lymphoma: an analysis of the German Hodgkin Study Group. Int J Radiat Oncol Biol Phys. 2008;71:1419–1424.
Fernandez J, et al. Manifestações cutâneas secundárias ao esquema ABVD. Hematologia. 2022;26(1):1–6.
Eich HT, Engenhart-Cabillic R, Hansemann K, et al. Quality control of involved field radiotherapy in patients with early-favorable (HD10) and early-unfavorable (HD11).
Hodgkin’s lymphoma: an analysis of the German Hodgkin Study Group. Int J Radiat Oncol Biol Phys. 2008;71:1419–1424.
Richardson SE, et al. The management of classical Hodgkin’s lymphoma: past, present and future. Adv Hematol. 2011;2011:1–17.
Halbsguth TV, et al. The unique characteristics and management of patients over 60 years of age with classic Hodgkin lymphoma. Curr Hematol Malig Rep. 2011;6:164–171.
Aridgides P, et al. A PET response-guided treatment of Hodgkin’s lymphoma: a review of the evidence and active clinical trials. Adv Hematol. 2011;2011:Article ID 309237.
Baxi SS, Matasar MJ. State-of-the-art issues in Hodgkin’s lymphoma survivorship. Curr Oncol Rep. 2010;12:366–373.
Farrell K, Jarrett RF. Molecular pathogenesis of Hodgkin lymphoma. Histopathology. 2011;58:15–25.
Siqueira VR, Soares TB, et al. Insuficiência respiratória aguda induzida por bleomicina. Hematol Transfus Cell Ther. 2022;44(S2):S1–S689.
Cassiano J, Silva ACP, et al. Bronquiolite obliterante com pneumonia em organização após uso de bleomicina em paciente com Linfoma Hodgkin. Hematol Transfus Cell Ther. 2023;45(S4):S1–S1006.
Thomas TS, Luo S, et al. Advancing age and the risk of bleomycin pulmonary toxicity in a largely older cohort of patients with newly diagnosed Hodgkin lymphoma. J Geriatr Oncol. 2020;11:69–75.
Jona A, Miltenyi Z, et al. Late pulmonary complications of treating Hodgkin lymphoma: bleomycin-induced toxicity. Expert Opin Drug Saf. 2014;13:1291–1298.